-
Laboratory Test
West Nile Virus, RT-qPCR
Pathogen test The RT-qPCR test detects the genome (RNA) of West Nile Virus (WNV). Sample 5 mL - blood - K3 EDT...
€61.50 -
Laboratory Test
Complete culture test
Parameter Bacteriological and mycological culture Includes antibiogram (if applied) Sample Aspirates, fluids, soli...
€39.98 -

Laboratory Test
Strangles Bacterial Culture
Pathogen test The bacterial culture will be reported positive if a beta-hemolytic Streptococcus species is grown a...
€30.75 -
Laboratory Test
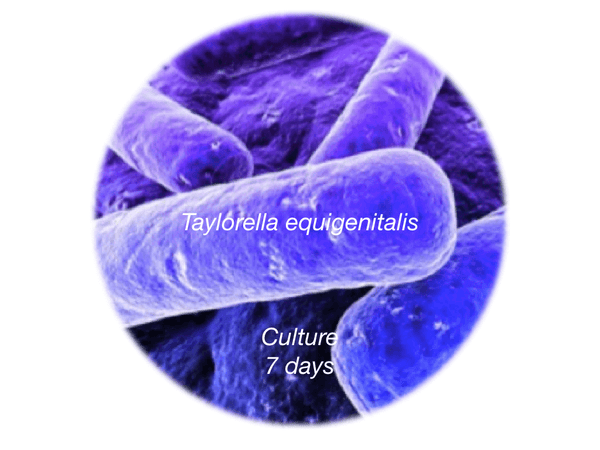
Contagious Equine Metritis Organism - CEMO, 7d culture
Pathogen test The culture test detects the presence of Taylorella equigenitalis, the most comum bacteria responsib...
€92.25 -

Laboratory Test
Equine uterine culture
Parameter Culture of the uterus Sample Uterine swab in special culture transport system Turnaround time 1-15 d...
€39.43 -
Laboratory Test
Borrelia burgdorferi, IFAT
Pathogen test IFAT for Borrelia burgdorferi, the pathogen responsible for the Lyme disease or Borreliose. IgG + ...
€55.17 -
Laboratory Test
Anaplasma phagocytophilum/ Erlichiosis by IFAT
Anaplasma phagocytophilum / Erlichiosis test by IFAT the bacterium (formerly known as Ehrlichia phagocytophila and ...
€55.17 -
Laboratory Test
Leptospira MAT
Pathogen test The microscopic agglutination test (MAT) is the reference test method for the serodiagnosis of leptosp...
€67.48 -

Laboratory Test
Canine COVID19 Molecular
Protect your pets from SARS-CoV-2 infection Dogs are susceptible to SARS-CoV-2 by reverse zoonosis. If you're infecte...
€65.00 -
Laboratory Test
Feline COVID19 Antibody
Protect your pets from SARS-CoV-2 infection Cats are susceptible to SARS-CoV-2 by a reverse zoonosis. If you have COV...
€30.00 -
Laboratory Test
Mycological examination
Culture Mycological examination (direct and culture) Sample fur skin other Turnaround time 15 to 30 days
€20.00 -

Laboratory Test
Canine COVID19 Antibody
Protect your pets from SARS-CoV-2 infection Dogs are susceptible to SARS-CoV-2 by a reverse zoonosis. If you have COV...
€30.00











