-

Laboratory Test
Equine uterine culture
Parameter Culture of the uterus Sample Uterine swab in special culture transport system Turnaround time 1-15 d...
€39.43 -

Laboratory Test
Copper
Parameter Copper Sample 5 mL - blood - serum tube Turnaround time 2 to 5 working days
€11.99 -
Laboratory Test
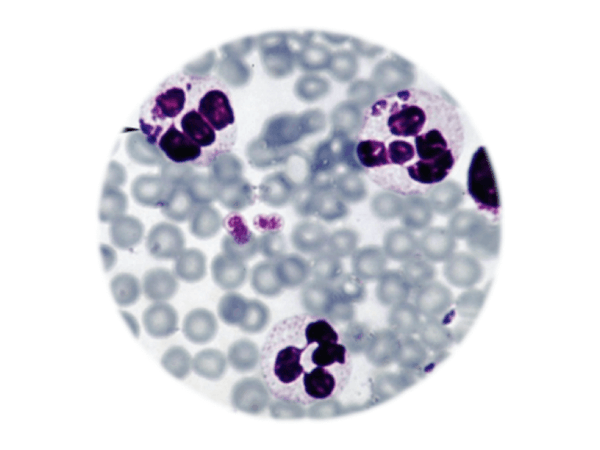
Anaplasma phagocytophilum/ Erlichiosis by IFAT
Anaplasma phagocytophilum / Erlichiosis test by IFAT the bacterium (formerly known as Ehrlichia phagocytophila and ...
€55.17 -
Laboratory Test
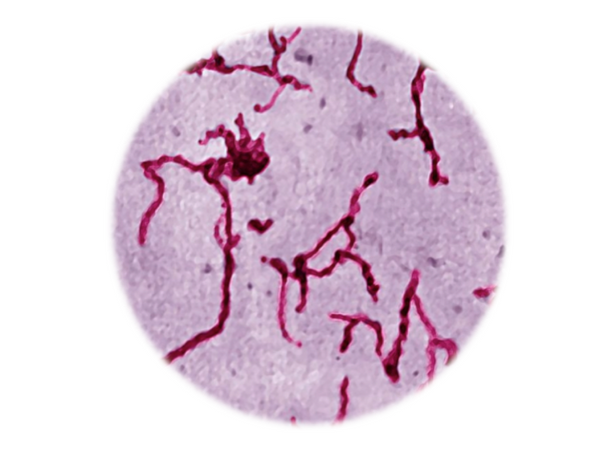
Leptospira MAT
Pathogen test The microscopic agglutination test (MAT) is the reference test method for the serodiagnosis of leptosp...
€67.48 -
Laboratory Test
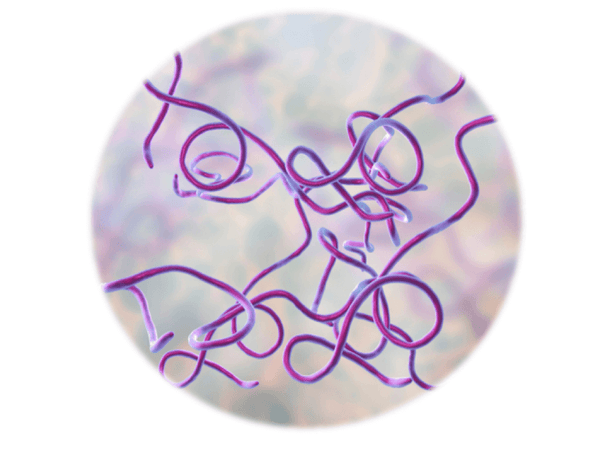
Borrelia burgdorferi, IFAT
Pathogen test IFAT for Borrelia burgdorferi, the pathogen responsible for the Lyme disease or Borreliose. IgG + ...
€55.17 -
Diagnostic Profile
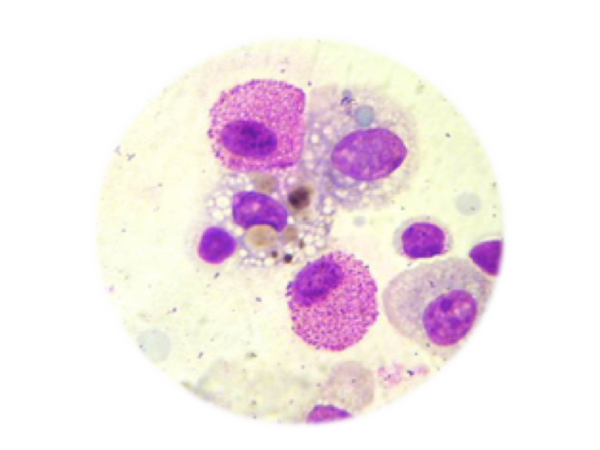
Equine Bronchoalveolar Lavage (BAL) Profile
Parameter Cytological, bacteriological and mycological analysis Antibiogram (if applied) Sample Equine Bronchoalve...
€67.65 -
Laboratory Test
Complete culture test
Parameter Bacteriological and mycological culture Includes antibiogram (if applied) Sample Aspirates, fluids, soli...
€39.98 -

Diagnostic Panel
Comprehensive Allergy Panel
About the Test – Comprehensive Allergy Panel The Comprehensive Allergy Panel evaluates sensitivity to a wide range o...
€547.04 -

Diagnostic Panel
Full allergy screening
Results Results are provided (reactive 0 to 5 ) for all allergens in all 4 allergen classes, with identification of...
€611.74 -
Diagnostic Panel
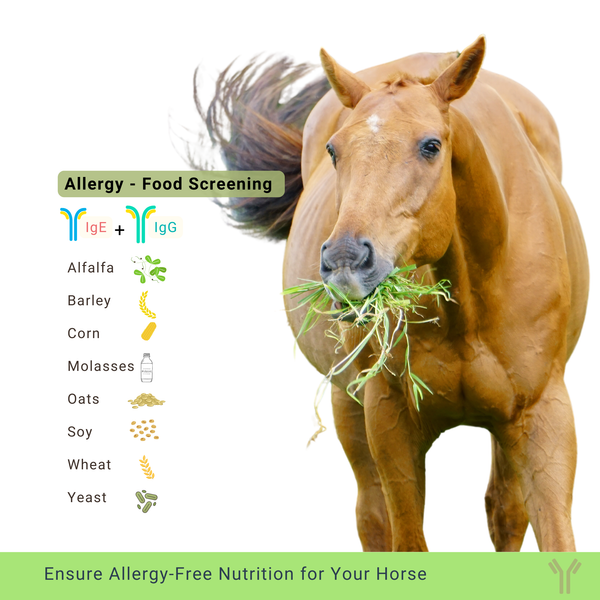
Allergy test for food allergens
Allergy testing Results: Results are given reactive/ non-reactive with identification of 8 different specif...
€281.25 -

Diagnostic Panel
Allergy test to feathers, hair and skin of other animals
Allergy testing Results: The results are provided as positive/negative results for each of the 6 allergens compose...
€179.00 -

Diagnostic Panel
Sweet Itch Allergy Testing
Why Test? Equine allergies are relatively common and can affect horses of any breed, age, or sex. Allergic reactions ...
€229.86











