-

Laboratory Test
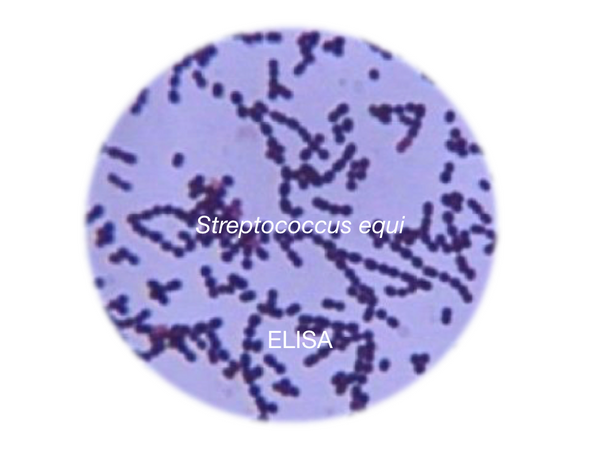
Strangles qPCR
About the Test The qPCR test detects the genome (DNA) of Streptococcus equi subspecies equi, the pathogen responsi...
€55.35 -
Laboratory Test
Equine Infectious Anemia - Coggins test, AGID
Pathogen test This is one of the internationally imposed tests in the import/export of live equines or semen/ova a...
€32.52 -

Diagnostic Profile
Equine Piroplasmosis cELISA
Equine Piroplasmosis is a serious tick-borne disease caused by Babesia caballi and Theileria equi....
€74.00 -
Laboratory Test
Glanders Burkholderia mallei qPCR
Pathogen test The PCR test detects the genome (DNA) of Burkholderia mallei, the bacteria responsible for Glanders...
€55.35 -
Laboratory Test
Dourine - Trypanosoma equiperdum, qPCR
Pathogen test The PCR test detects the genome (DNA) of Trypanosoma equiperdum, the pathogen responsible for Douri...
€55.35 -
Laboratory Test
Equine Herpesvirus Type 4, qPCR
Pathogen test qPCR test: Detects the genome (DNA) of Equine Herpesvirus Type 4 (EHV-4). ...
€55.35 -
Laboratory Test
Equine Herpesvirus Type 1, qPCR
Pathogen test qPCR test: Detects the genome (DNA) of Equine Herpesvirus Type 1 (EHV-1). ...
€55.35 -
Laboratory Test
Strangles ELISA
Pathogen test The iELISA test detects specific antibodies to Streptococcus equi subs. equi, the pathogen (bacteri...
€43.05 -
Laboratory Test
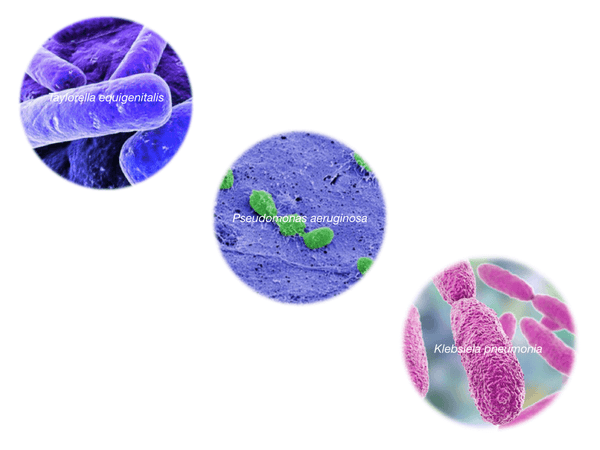
Contagious Equine Metritis (CEM), qPCR
Screening of 3 pathogens responsible Contagious Equine Metritis (CEM): Taylorella equigenitalis, qPCR Pseudomo...
€99.30 -
Laboratory Test
African Horse Sickness, ELISA
Pathogen test The ELISA test detects antibodies to the African Horse Sickness Virus (AHSV). Sample 5 mL - bloo...
€30.75 -

Diagnostic Profile
Respiratory signs profile
Pathogen profile Screening of 5 pathogens responsible for respiratory disease in equines: ...
€150.00 -
Laboratory Test
VE Vesicular Stomatitis RT-qPCR
Pathogen test The RT-qPCR test detects the genome (RNA) of Indiana and Jersey virus strains responsible for Vesicu...
€61.50











